One Million and One Nights: What Sleep Reveals About Life in Senior Living
Since early 2024, Teton has been tracking residents' sleep. Here are stories from more than a million resident nights, and how the increased visibility is helping care staff provide more personalized and proactive care.
June 2026·Insights
Sleep is one of the most important health indicators for delivering proactive and personalized care. Yet in most senior living communities, staff have little visibility into how residents are actually sleeping.
Care teams can now see how every resident actually sleeps through the night. After tracking more than a million resident-nights, we have found that sleep patterns vary dramatically between residents, that routine checks can materially disrupt rest, and that combining sleep with movement and breathing data helps care teams identify changes that would otherwise remain invisible. In the senior living communities using Teton, residents now sleep on average nearly an hour longer each night, and experience an 8% increase in sleep efficiency compared to before go-live. Wake-ups fall in proportion to how disturbed sleep was at baseline: large in the few high-baseline sites, modest across more typical residents, and absent where wake-ups were already low. You can find all the details of our analysis here. We have also found that residents with irregular sleep are 1.5 times more likely to fall, in our analysis of 2,000 falls; see more here.
1,000,000+
resident-nights tracked
since early 2024
65%
of residents nap
median 25 min · 26% in a chair
2
median bed exits a night
median 1 bathroom visit
Teton's contactless sleep tracking provides continuous, real-time insights into residents' sleep patterns, so care staff can identify changes early and adapt care to individual needs. In this post, we explore why sleep is such an important health metric and share insights from our first million and one resident-nights, and show how continuous sleep tracking can support better care delivery.
Why sleep remains a blind spot in care delivery
Sleep plays a major role in overall health, and this remains true as we age. However, it can become harder to get sufficient sleep later in life as sleep becomes shorter and lighter, with more frequent wake-ups and sleep disorders becoming more common. The recommended amount of sleep may change, but getting enough good sleep is important for everyone, to ward off future problems and to help manage existing ones [1], [2].
In a senior living setting, this makes sleep a valuable thing to track over time. Consistent, restful nights tend to reflect stable health and comfort, while sudden changes such as more wake-ups, an irregular sleep schedule, or unusually long sleep can point to discomfort, illness, or decline, and give care teams an early opportunity to check in [3].
The problem is that existing approaches are often difficult to use continuously in senior living. Clinical methods are too invasive, wearables are impractical for continuous use, and bed-based sensors are inflexible and miss sleep outside the bed.
Teton sleep tracking gives staff visibility into sleep patterns
Teton tracks resident sleep in real time and gives visibility into where a resident sleeps, when they sleep, and how they sleep. It tells care staff if a resident was likely woken by staff or on their own. It surfaces changes in their sleep schedule to help staff understand when a resident usually sleeps, how often they wake during the night, and which residents prefer a nap in the afternoon. Teton sleep tracking has been live since early 2024, and we have now tracked more than one million resident-nights. The charts below are based on a three-week snapshot of that data, giving a clear, current picture of how residents sleep. You can find the full methodology and per-metric details in the appendix.
Lying in bed
Sitting in bed
Sitting on bed edge
Standing on floor
Sleeping, lying in bed
Sleeping, sitting in bed
Sleeping, sitting in chair
In bathroom
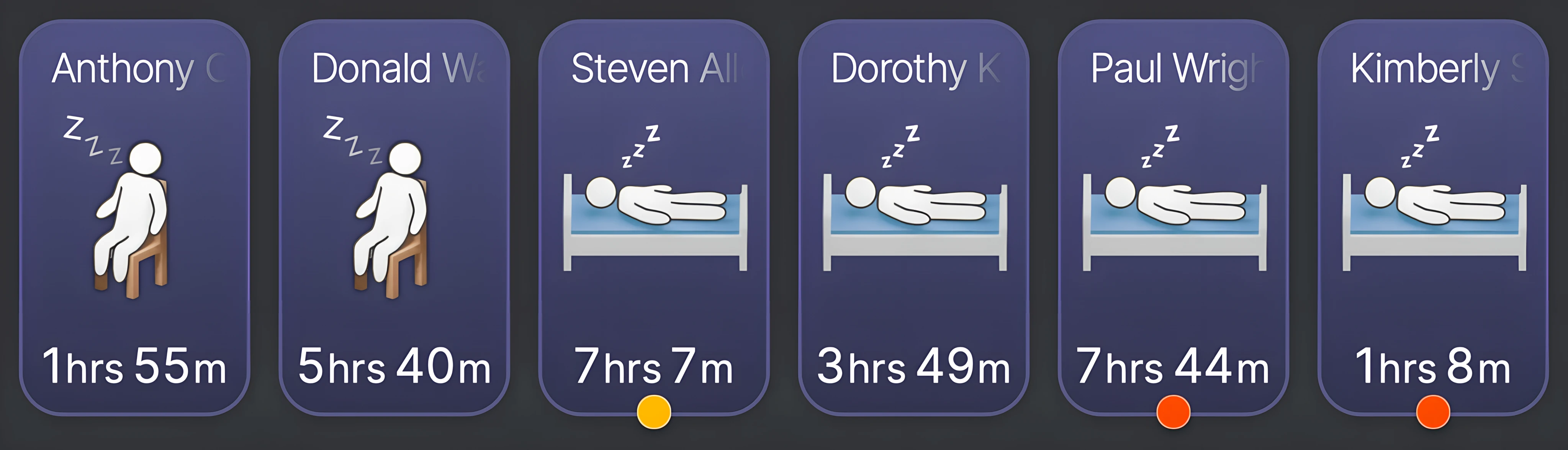
Teton recognizes each resident's position and state in real time.
Real-time overview
Understanding how residents sleep improves quality of life for both residents and care staff. One of the simplest wins is leaving sleeping residents undisturbed: knowing who is already awake lets staff reorder their morning visits and time night rounds to minimize unnecessary wake-ups. It matters a lot for regular residents, and even more for frail or vulnerable ones, like those with dementia [4]. An interrupted night's sleep can shape the entire day, and care has to be adjusted accordingly, but if you only realize it after the fact, it's too late.
Teton provides a real-time overview of who is asleep.
Amount of sleep
Sleep data gives staff something concrete to point to, backing up a note that someone “seemed tired” and enriching handovers and conversations with families. And it lets them check whether changes in daily routines actually work. When one resident was lying awake for an hour or two before falling asleep, staff shifted the bedtime routine later and could follow the data over the following nights to confirm it helped.
Total daily sleep
Share of resident-nights by total sleep per 24 hours, all residents over three weeks.
On average residents sleep just under eight hours a day, but sleep patterns follow a fairly even distribution from about four hours a night up to eleven. This shows that sleep is individual, and it has motivated our personalized, adaptive UI.
Personalized sleep UI
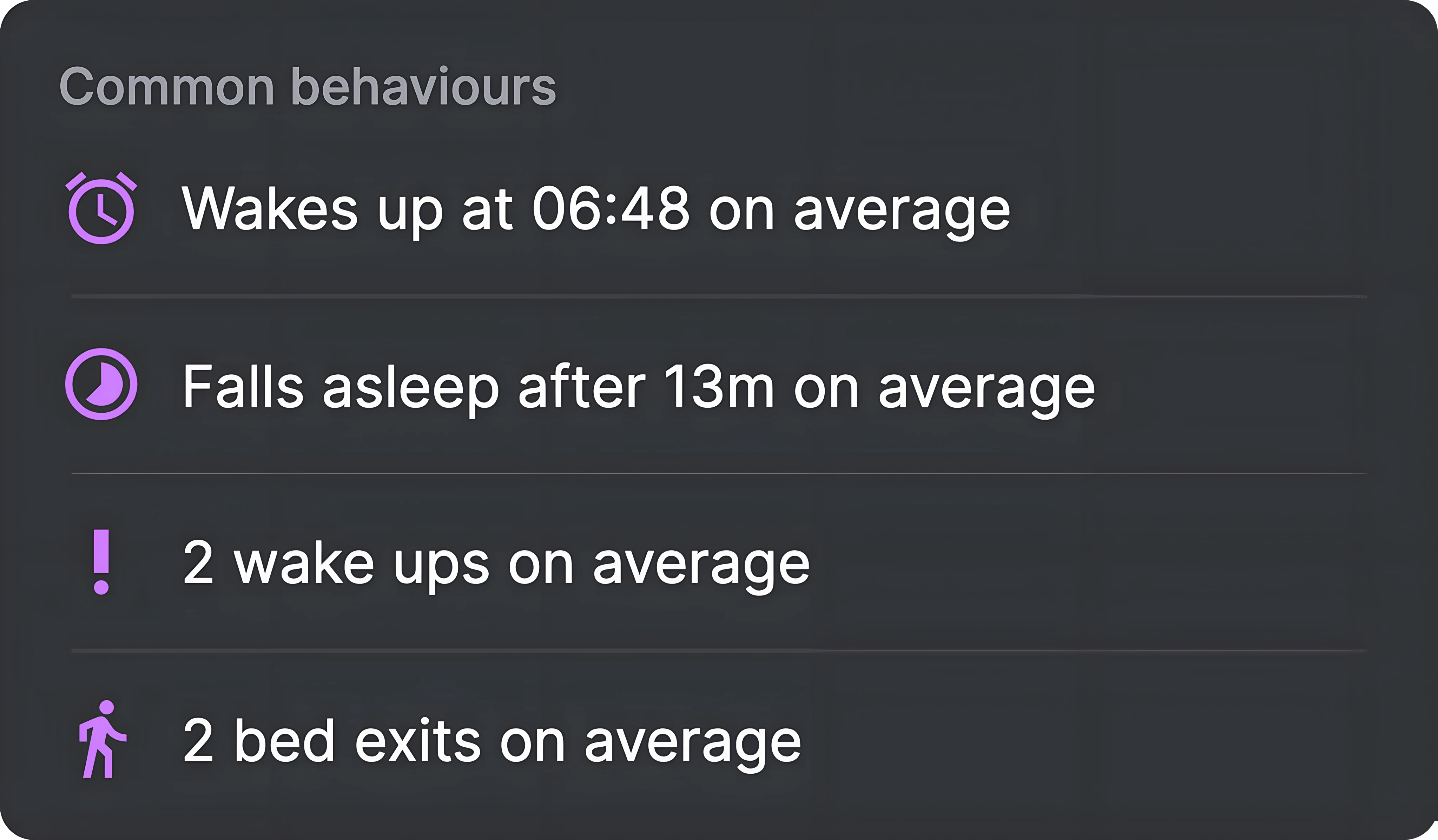
Our sleep widget shows how much a resident sleeps each day, when they went to bed, and when they woke up. From the widget, you can see whether a resident took a nap on a given day or not.
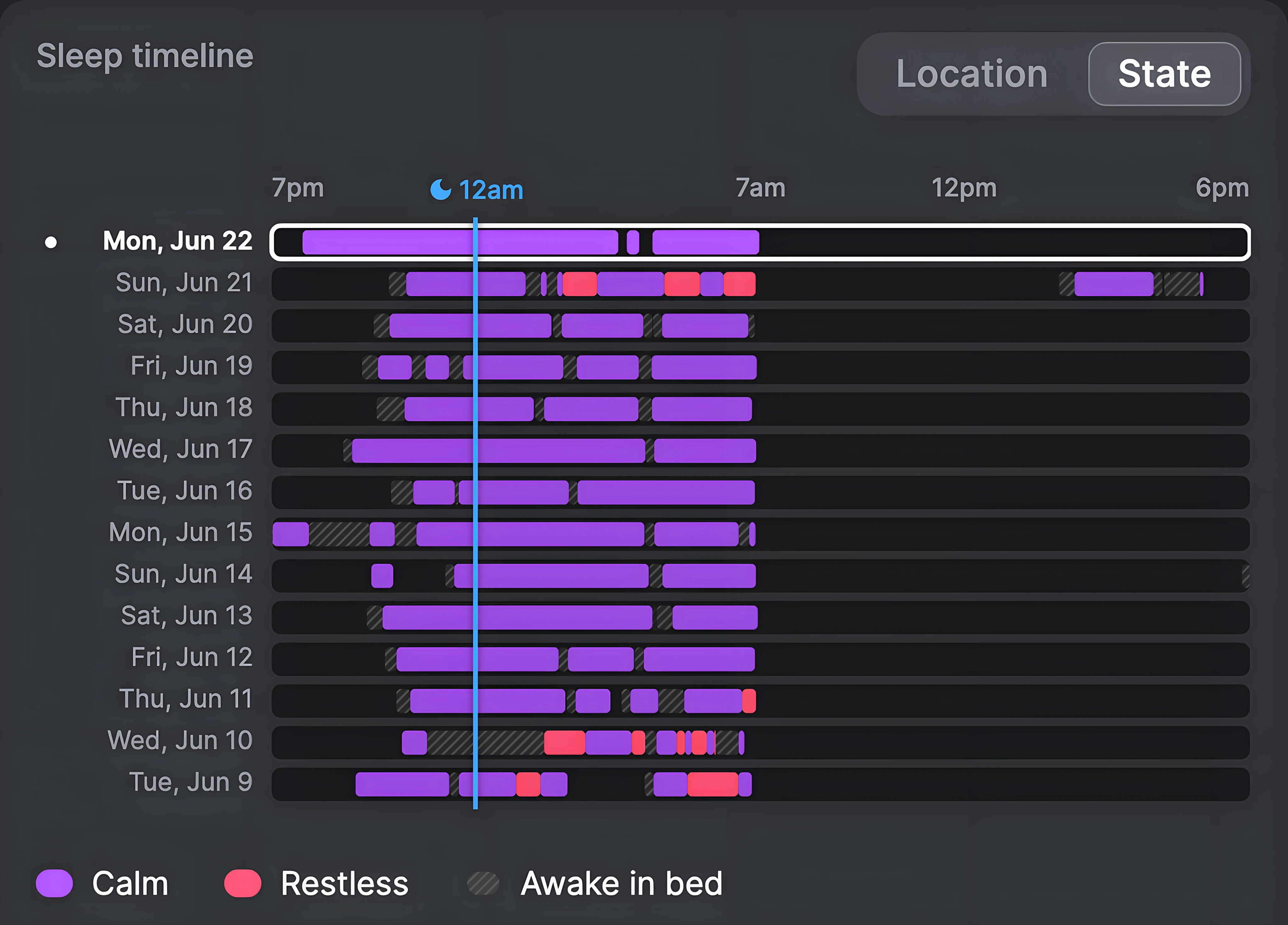
In this example, the resident sleeps a bit more than eight hours on average. The real insight comes from combining that aggregate with the day-to-day schedule below. This resident has a fairly consistent sleep pattern, with few wake-ups on most days.
The timeline shows each night's regular and restless sleep, and awake-in-bed periods, the day-to-day detail behind the average.
Sleep location
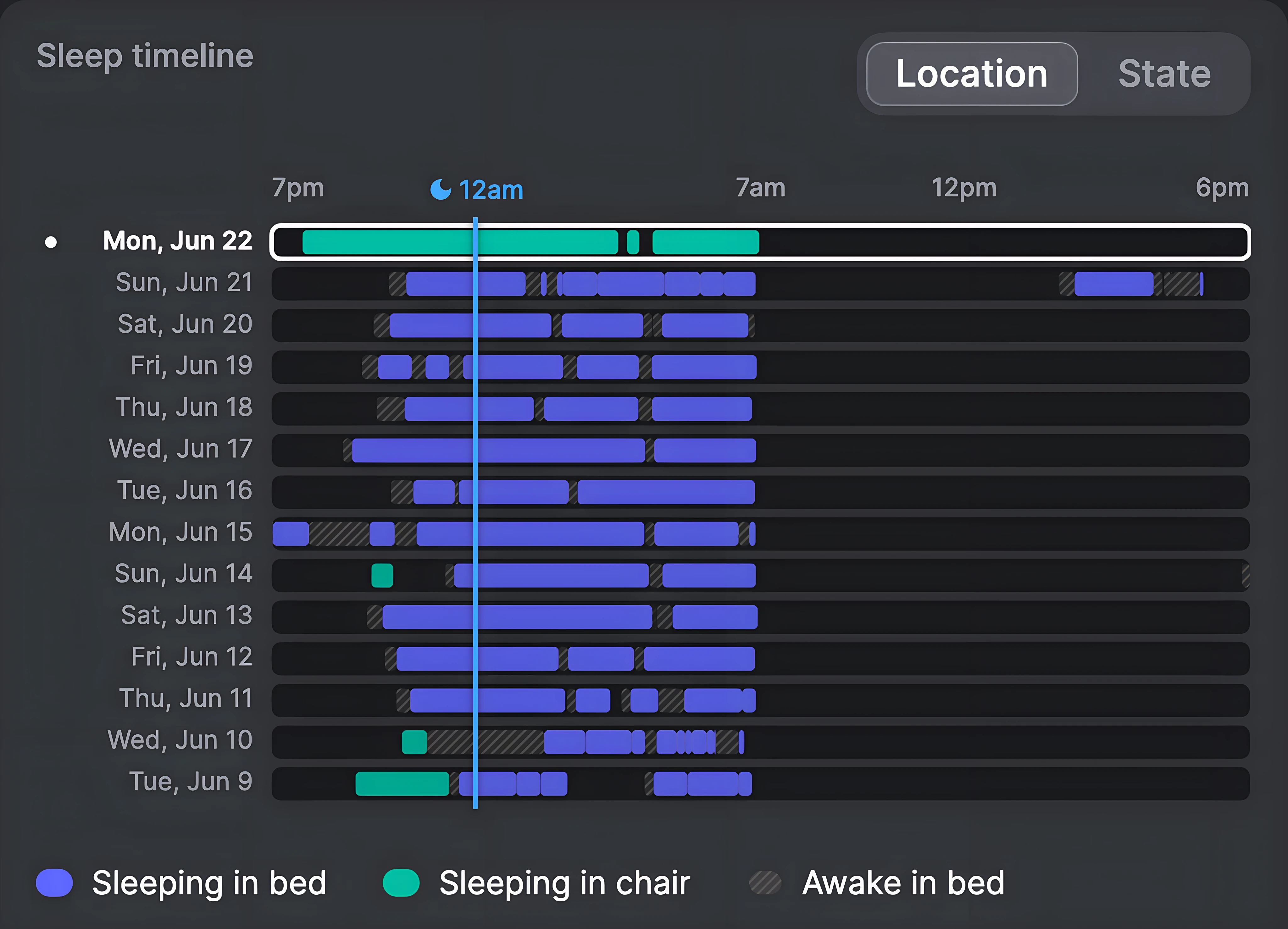
The Teton system tracks sleep both in bed and when residents sit in chairs. The resident example above hides a detail we would miss without chair support. Switching the timeline to “Location” shows that several of this resident's more unusual nights also involved time in a chair. On June 9 and 10 they slept in stretches broken by long gaps, with a short spell in the chair early each evening. On June 22 they went to bed much earlier and spent the entire night in the chair rather than the bed.
The same timeline switched to Location: green marks time slept in a chair, including the full chair night on June 22.
Looking across our population of residents, sleeping in a chair for most of the night is fairly rare. Over the three-week period, only 3% of resident-nights were primarily spent in a chair. About 9% of residents had at least one night where they slept in a chair instead of in bed, but only 1% are primarily chair sleepers, doing it nearly every night. We also found cross-continental differences: residents at our US sites are four times more likely to sleep in chairs than residents at our European sites, which points to cultural and behavioral differences.
Bed versus chair
Share of resident-nights spent mostly in bed or in a chair, across our three-week analysis.
97.0%
In bed
3.0%
In a chair
Sleep schedule
On the timeline, a regular schedule shows up as blocks landing in the same place each day, while an irregular one drifts around. A typical night runs from around ten in the evening to about eight in the morning, with plenty of variation between residents.
Across all sites, some average trends emerge. Residents tend to go to bed around 10:00 PM, and once in bed it takes around 20 minutes to fall asleep. The sleep data lets us see morning routines too, and the patterns are similar, with residents generally waking around 8:00 AM and getting out of bed about 75 minutes later, though that does not mean the night passed without interruptions in between. The figure below shows the distribution of when residents go to bed, fall asleep, wake up, and get out of bed.
Bedtimes and wake times
When the four sleep-schedule events happen, in department local time, on a shared 7 PM to noon axis.
Went to bed
Fell asleep
Woke up
Got out of bed
But keeping a steady schedule doesn't always mean sleeping well. Two residents can go to bed and wake at the same time and still have very different nights: one sleeps straight through while the other's is fragmented.
Sleep disturbances
Getting the optimal amount of sleep becomes less important if it's interrupted by frequent wake-ups and bed exits. Residents wake up and even leave their beds for various reasons, such as wandering around the room or using the bathroom. They can remain awake for extended periods or return to bed immediately. The first step in helping residents achieve more restful nights is to acknowledge the problem and identify when it occurs. The Teton system can assist by distinguishing between wake-ups caused by staff in the room and spontaneous ones. It can also track when residents fall asleep and leave their beds, possibly to use the bathroom or leave the room. In a comparison of the time before and after implementing Teton at senior living communities, we see almost an hour more sleep and an 8% increase in sleep efficiency. Wake-ups fall in proportion to how disturbed sleep was at baseline: large in the few high-baseline sites, modest across more typical residents, and absent where wake-ups were already low. You can find the full analysis here. Sleep efficiency is the ratio of time spent asleep to time spent in bed, and is considered a simple proxy for sleep quality [5].
“
Teton is worth its weight in gold. It's a tool I use a great deal, and it gives me peace of mind on the night shift. I can see when it's best to go in and check on the residents, and when to let them sleep. I hope we'll get Teton in even more rooms.
Lotte Nielsen
Night shift, Akutpladserne på Marskvej
These disturbances matter beyond the night itself. Sleep regularity, how consistently a resident falls asleep and wakes at the same times, tracks closely with falls. In our fall analysis, The Anatomy of 2,000 Falls, we found that residents with irregular sleep are 1.5 times more likely to fall. In that post you can learn more about how sleep, movement transitions, and inactivity together shape a resident's risk of falling.
Comparing hospital patients with senior living residents
The product is available in both senior living communities and hospitals, and the difference between the two is striking. The median hospital patient sleeps about an hour less a night and spends roughly four hours longer in bed, so their sleep efficiency drops sharply, with more frequent wake-ups through the night.
Senior living versus hospital
Median per resident-night over the three-week window.
Senior living Hospital
Total sleep per day
8h 7min
6h 48min
Time in bed per day
11h 55min
16h 2min
Sleep efficiency
70%
44%
Night wake-ups
5
6
This makes sense if you think about the two settings. Once a resident has settled into a senior living community, it is home. The place is familiar, the routine is known, and it is their own bed and the same faces every day. A hospital is almost the opposite. It is an unfamiliar room, often with an uncertain or worrying outcome, and the nights are busier and noisier, with more clinical activity around the bed such as checks, rounds, and interventions. None of that helps people sleep deeply or without interruptions. The numbers are not a verdict on either setting, but are roughly what you would expect when one environment is built around being at home and the other around being treated.
Visibility enables proactive and personalized care
One recent case comes from a senior living community, and shows what happens when sleep and breathing data are read together. One resident there lives with COPD and cannot communicate verbally, so staff had no way to know how badly his breathing was disrupting his sleep. The data showed repeated stretches of little rest, until chair tracking revealed he barely slept in bed but slept through the night on his couch, where his upper body was elevated enough to breathe easily. Staff brought this to his doctor, and the combination of high breathing rates and poor sleep prompted fuller examinations that uncovered lung abnormalities needing urgent attention. He was given a bed that raised his upper body the same way, and staff can now ask far more targeted questions about how he is feeling, even without him speaking.
By surfacing outliers for staff, the system lets them take a closer look when needed and improve the care a resident receives. Sleep estimates are useful alone, but read alongside our other signals and staff's in-depth knowledge, together they can help surface hidden problems and improve quality of life for residents.
How Teton understands a resident's sleep
The Teton sensor detects every person in the room, including residents, visitors, and staff, and classifies what they are doing ten times per second, using only on-device AI processing with no video data leaving the device. You can read more in our post, How Teton Sees the Room.
When a resident is lying or sitting in a bed or chair, the Teton system automatically starts estimating the current sleep state of the resident without requiring any contact-based sensors. The sleep estimation is done locally on the device, similarly to the rest of the AI processing we do. Our sleep estimation model takes two signals as input: the resident's motion pattern and their breathing.
Motion
Our AI estimates the 3D location of a resident's position over time. The resident's movement maps coarsely to their sleep state, and provides a strong signal when a resident is moving around in bed, shuffling between positions, or experiencing periodic limb movements.
2× speed
Awake in bed
2× speed
Awake in a chair
In the above two examples we see how Teton follows each resident's position and movement while they are awake. In bed they lie down and settle into a comfortable position; in a chair they sit down and recline the chair toward horizontal.
Breathing rate
The other main source of information is breathing waveforms, derived remotely from chest movement and serving as a proxy for the respiratory effort normally captured in a sleep study with chest and abdominal belts. Breathing data contains a wealth of information that can be valuable for sleep staging, in particular for telling wakefulness and sleep apart [6].
2× speed
ESTIMATED ON DEVICE
Breathing rate
16breaths/min
−14s−7snow
Sleeping in chair
In this example we see the anonymized view of a resident napping in their chair; on the right is their breathing, estimated on-device from the movement of the chest with no wearable or contact, where each rise and fall is one breath. Breathing complements the coarser motion signal rather than repeating it: motion is always available but low in detail, whereas breathing is far richer yet only readable while the resident stays still, so when one fades the other tends to carry the information.
Breathing rate estimation is shown here to illustrate the signal behind sleep tracking. Live breathing rate monitoring is not a feature in any of Teton's products.
Three states of sleep
We estimate three different states: awake, asleep, and restless sleep. The restless sleep state derives from a need rather than a clinical term. As you age, your sleep becomes lighter and more fractured, and what might look like someone awake in bed for a younger adult can be part of a regular night's sleep for an elderly person. Reliably distinguishing between clinical sleep stages in an elderly population with a contactless sensor is extremely difficult outside a controlled sleep-lab environment, but telling normal sleep apart from restless sleep is not. Being able to identify periods of restless sleep can help staff launch investigations into a resident's sleep health and decide on possible interventions. We characterize our sleep states this way:
Awake: characterized by more movement, and a rapidly changing breathing signal if there is any signal at all. Remember, the absence of a breathing signal in a remote estimation setting is not the same as the absence of actual breathing.
Asleep: characterized by a primarily stable breathing signal and little to no movement, with the occasional shift in sleeping position.
Restless sleep: characterized by a somewhat stable breathing signal with periodic movement of one or more limbs.
To connect our sleep tracking to well-known methods, it can be considered an extended form of actigraphy. Actigraphy is a continuous, non-invasive method for tracking sleep using accelerometer data, typically collected from a wristwatch-like device worn by patients. Usually the data is processed offline after collection and analyzed by a medical professional or an algorithm to determine whether a patient was sleeping or awake [7]. We employ the same principle of using human motion as a reliable proxy for sleep, but we extend it by incorporating breathing data as well, and we run everything live, on-device with no video material leaving for offline processing.
From sleep data to better care
Sleep is not just a background metric of daily life in senior living. It is a continuous, sensitive signal of health, comfort, and change. Yet in most senior living communities it has been largely invisible in everyday care practice. By turning sleep into something that can be observed in real time and over long periods, care teams gain a new layer of understanding of their residents' wellbeing.
At scale, these patterns move beyond individual nights and become actionable insight, helping staff prioritize attention, reduce unnecessary disturbances, and track interventions. In doing so, sleep becomes a practical, everyday input into delivering more proactive, personalized care.
References
[1]P. Tatineny, F. Shafi, A. Gohar, and A. Bhat, “Sleep in the Elderly,” Missouri Medicine, vol. 117, no. 5, pp. 490–495, 2020.
[2]J. Li, M. V. Vitiello, and N. S. Gooneratne, “Sleep in Normal Aging,” Sleep Medicine Clinics, vol. 13, no. 1, pp. 1–11, Mar. 2018, doi: 10.1016/j.jsmc.2017.09.001.
[3]O. Itani, M. Jike, N. Watanabe, and Y. Kaneita, “Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression,” Sleep Medicine, vol. 32, pp. 246–256, Apr. 2017, doi: 10.1016/j.sleep.2016.08.006.
[4]A. L. Snow et al., “Enhancing sleep quality for nursing home residents with dementia: a pragmatic randomized controlled trial of an evidence-based frontline huddling program,” BMC Geriatrics, vol. 21, no. 1, p. 281, Dec. 2021, doi: 10.1186/s12877-021-02189-8.
[5]C. Sakal, T. Li, J. Li, C. Yang, and X. Li, “Association Between Sleep Efficiency Variability and Cognition Among Older Adults: Cross-Sectional Accelerometer Study,” JMIR Aging, vol. 7, pp. e54353–e54353, Apr. 2024, doi: 10.2196/54353.
[6]D. Krauss et al., “Incorporating respiratory signals for machine learning-based multimodal sleep stage classification: a large-scale benchmark study with actigraphy and heart rate variability,” SLEEP, vol. 48, no. 9, p. zsaf091, Sep. 2025, doi: 10.1093/sleep/zsaf091.
[7]M. R. Patterson et al., “40 years of actigraphy in sleep medicine and current state of the art algorithms,” npj Digital Medicine, vol. 6, no. 1, p. 51, Mar. 2023, doi: 10.1038/s41746-023-00802-1.
Appendix
The full baseline-to-go-live analysis behind the improvement figures, with the methodology, per-metric results and the wake-up sub-analysis.