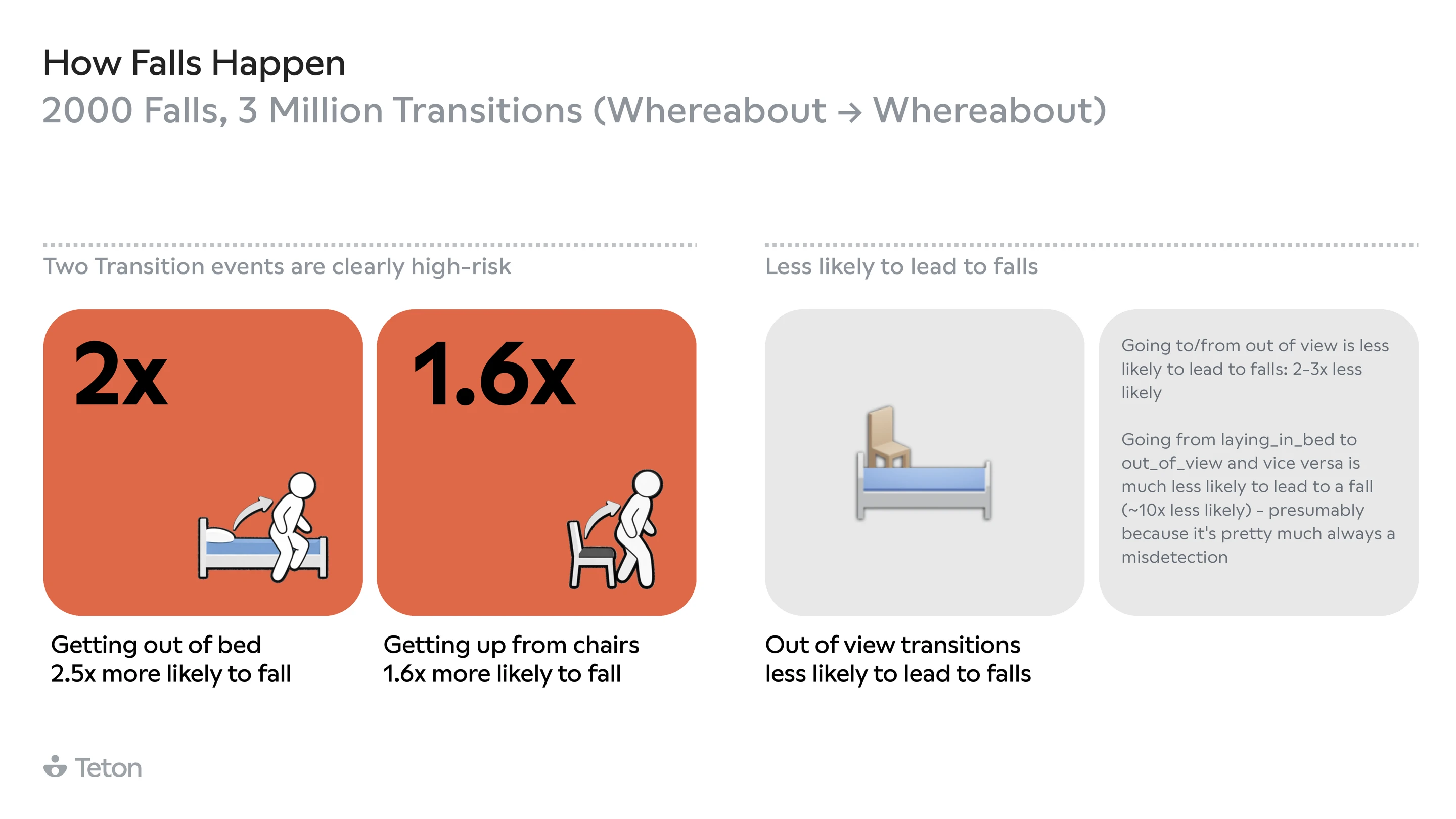
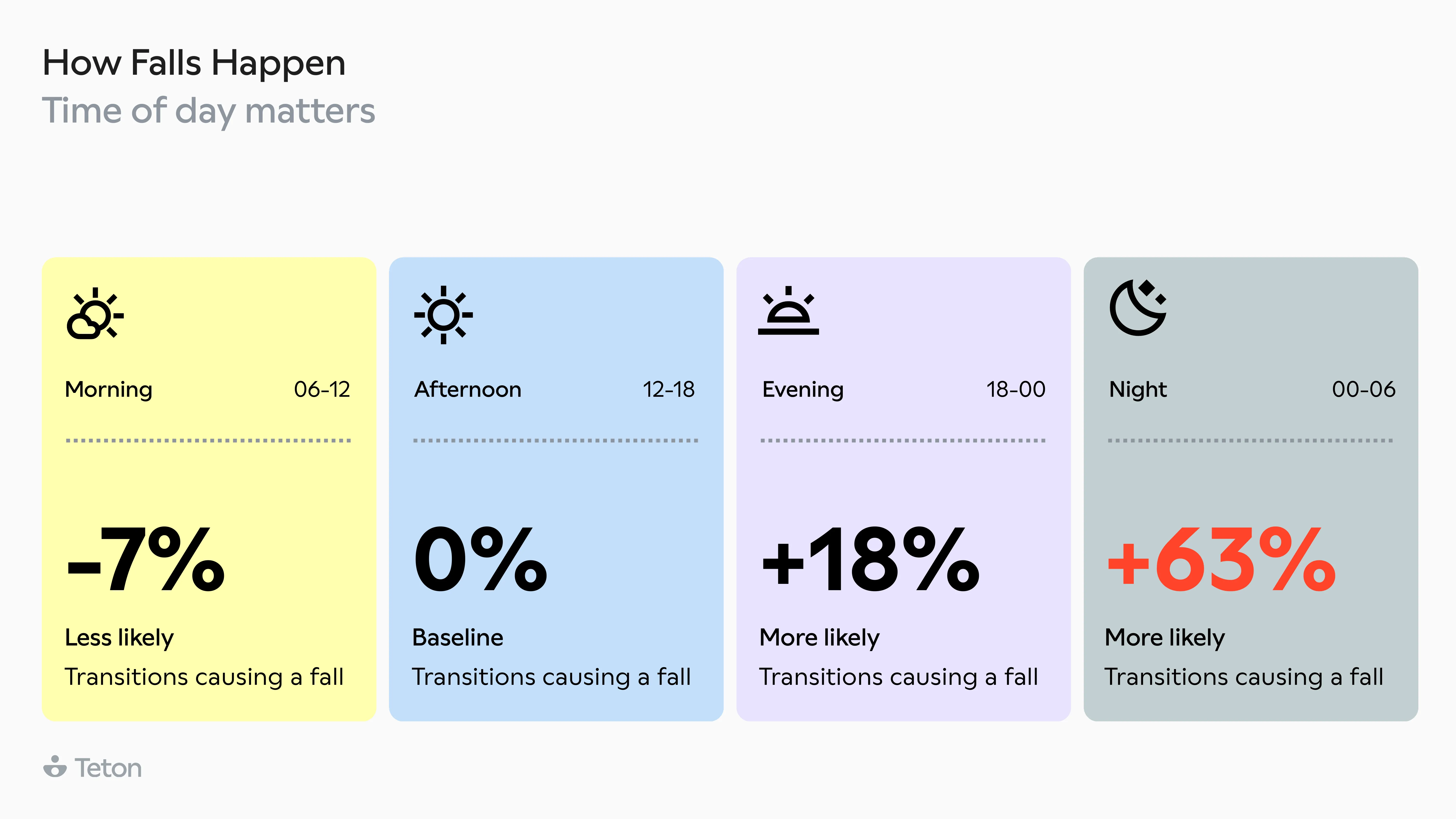
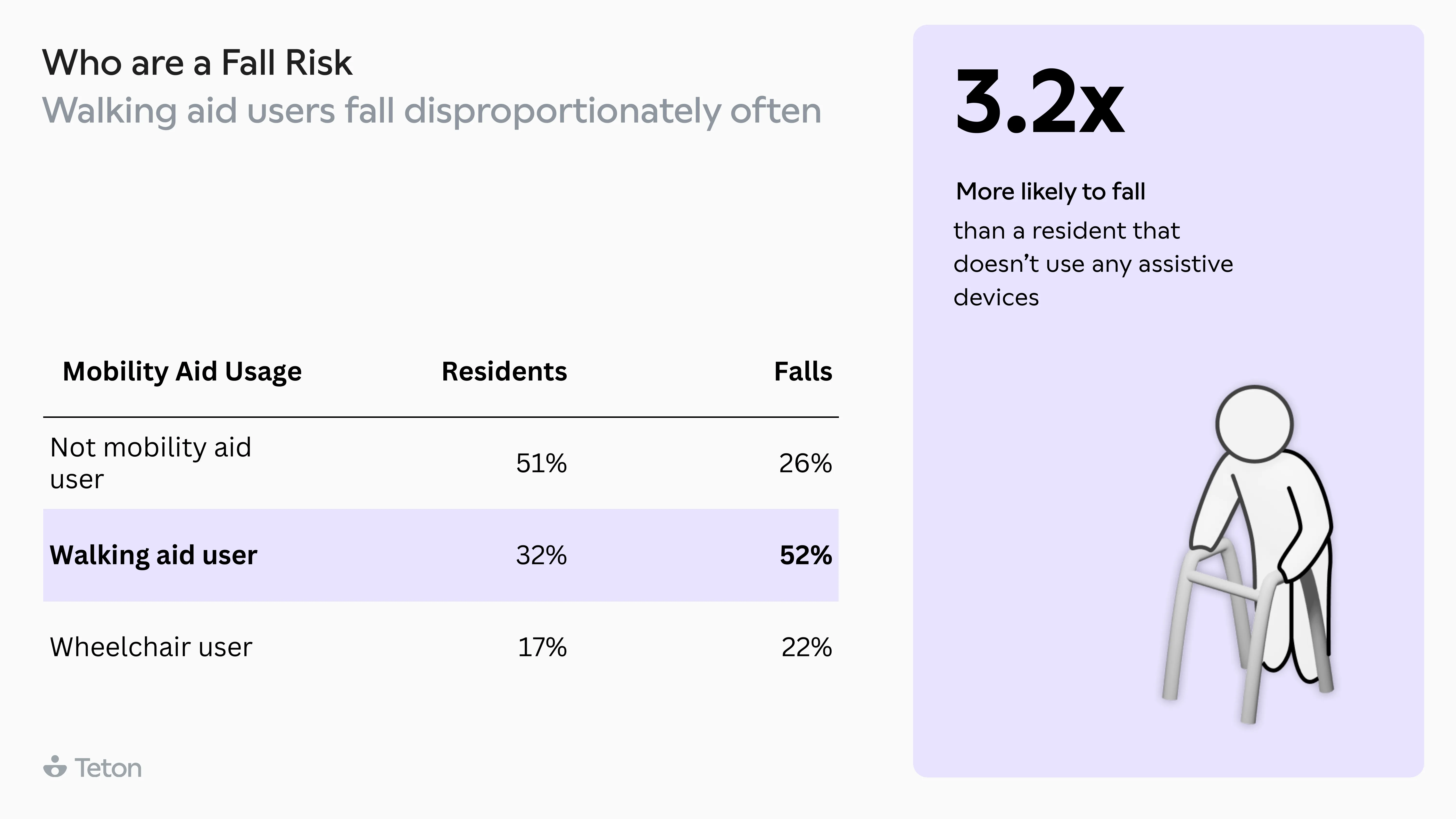
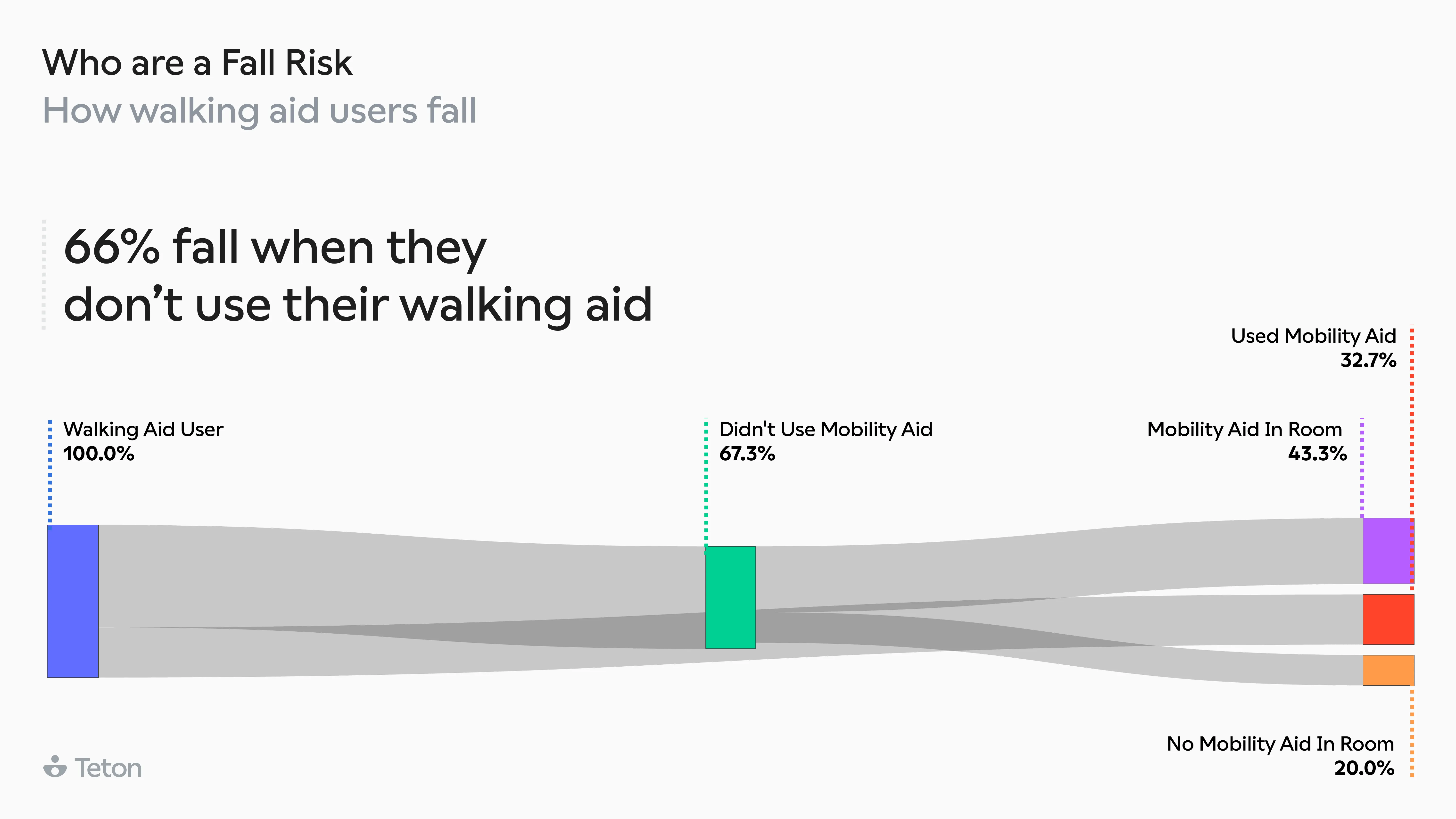
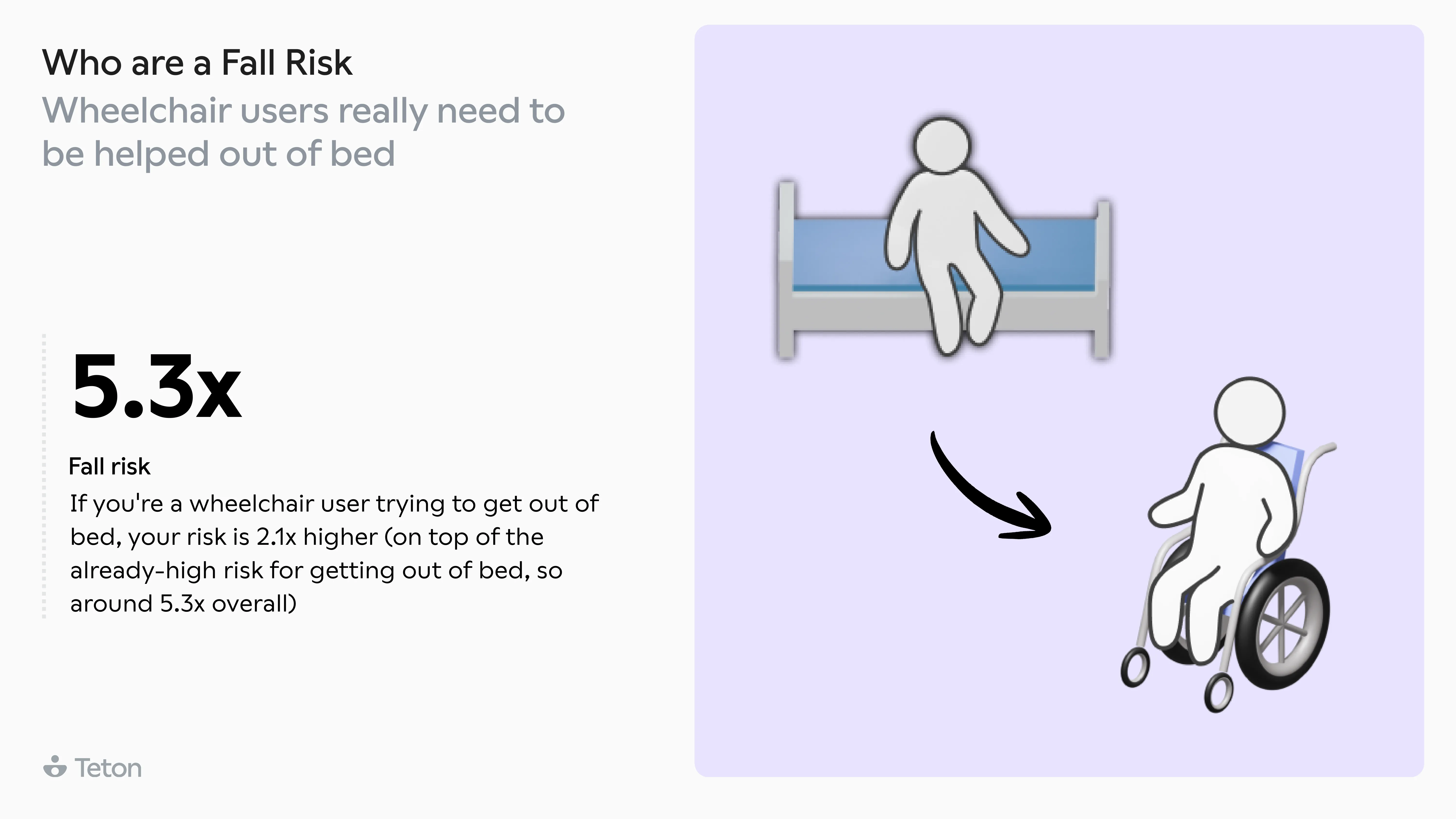
Getting out of bed is 2.5x more dangerous than any other movement. The same transition at 3 AM is 63% more likely to end in a fall than at 3 PM. Walking aid users make up 32% of residents but account for 52% of all falls, and two-thirds of those falls happen when the aid isn't even being used. The biggest finding? 79% of falls in care settings are avoidable.
These aren't estimates. They come from 2,000 confirmed falls and 3 million state transitions recorded by Teton's monitoring system across care settings in the United States, Denmark, the United Kingdom, and Switzerland. We analysed all of it to answer a practical question: what actually precedes a fall, and what can we do about it? Here is everything we found.